

Your shopping cart is empty.
3D Printed Tracheoesophageal Fistula and Oesophagus Atresia





 Handling Guidelines for 3D Printed Models
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer






















































3.0 lb





3D Printed Tracheoesophageal Fistula and Oesophagus Atresia
Item # MP2059
$281.00
$313.00
You save $32.00
Need an estimate?
Click Add To Quote

Features & Specifications
-
 by
by
A trusted GT partner -
 3D Printed Model
3D Printed Model
from a real specimen -
 Gov't pricing
Gov't pricing
Available upon request
 by
by 
About This Item
3D Printed Tracheoesophageal Fistula and Oesophagus Atresia
Clinical History
A 32-year-old female G3P0 (gravida 3, para 0‘ – i.e., has had two pregnancies,
with neither of the embyros surviving to a gestational age of 24 weeks) presents in preterm labour at 25 weeks
gestation. The GP had noted an increased fundal height at 30cm one week prior, but the mother had refused prenatal
testing or ultrasound, and was lost to follow up. She d
Frequently Bought Together
Total Price: $1,562.91 $1,506.91
- This item: 3D Printed Tracheoesophageal Fistula and Oesophagus Atresia $313.00 $281.00
- Brayden CPR Training Manikin $495.00 $471.00
- Pediatric 4 Vessel Ultrasound Training Block $754.91
Total Price: $1,562.91 $1,506.91

3D Printed Tracheoesophageal Fistula and Oesophagus Atresia
Clinical History
A 32-year-old female G3P0 (gravida 3, para 0‘ – i.e., has had two pregnancies,
with neither of the embyros surviving to a gestational age of 24 weeks) presents in preterm labour at 25 weeks
gestation. The GP had noted an increased fundal height at 30cm one week prior, but the mother had refused prenatal
testing or ultrasound, and was lost to follow up. She delivered a live born male baby. Examination of the baby noted
polydactyly, imperforate anus, excessive drooling, and a loud pan-systolic murmur. A single umbilical artery was
noted in the umbilical cord. The baby had difficulty feeding with increasing respiratory distress. The baby died 2
days later from aspiration pneumonia.
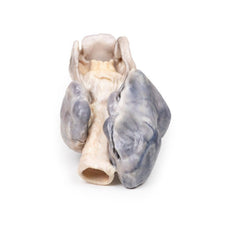
Pathology/Specimen Details
The specimen comprises the tongue, larynx, trachea, bronchi, both
lungs and oesophagus of the foetus. The trachea and bronchi have been divided in the midline. A fistula is present
just above the bifurcation at a communicating fistula can be seen connecting the distal oesophagus to the trachea
(arrow). This is an example of a Type C Tracheoesophageal Fistula (oesophageal atresia with distal tracheoesophageal
fistula). It is difficult to discern if the oesophagus ends as a blind pouch at the lower extent of the specimen.
Further Information
Tracheoesophageal Fistula (TEF) is a common congenital abnormality occurring
in about 1 in 4000 live births. TEF usually occurs with oesophageal atresia (sometimes abbreviated to EA, reflecting
the US spelling of ‘esophagus’). TEF are classified according to their anatomical configuration. Type C is the most
common configuration; as described above, in which oesophageal atresia with distal tracheoesophageal fistula making
up 86% of cases. TEF occurs without oesophageal atresia in only 4% of cases, Type E.
TEF and oesophageal atresia
are caused by defective lateral septation of the foregut into the oesophagus and trachea. It is believed that a
defect in epithelial-mesenchymal interactions causes failed branching of a lung bud branch which becomes the fistula
tract. It is associated with VACTERL (vertebral defects, anal atresia, cardiac defects, TEF, renal anomalies, and
limb abnormalities) or CHARGE syndrome (Coloboma, Heart defects, Atresia choanae, Growth retardation, Genital
abnormalities, and Ear abnormalities).
Oesophageal atresia can be seen on prenatal ultrasound as polyhydramnios, absent/collapsed stomach, and proximal
oesophageal pouch dilation. EA with TEF can be more difficult to see on ultrasound as fistula allows fluid flow into
the stomach. Polyhydramnios occurs in one third of cases of EA with distal TEF. Postnatal symptoms vary on the
configuration of the fistula. These include excessive drooling, respiratory distress, difficulty feeding and
choking. Reflux of gastric contents can lead to aspiration pneumonia as in this case.
Diagnosis can be made by
failing to pass a nasogastric tube into the stomach along with X-ray imaging. Fluoroscopy with contrast can be used
for more indeterminate cases. For milder cases diagnosis may be made later with endoscopic investigation. Treatment
involves surgical correction of the defects. Prognosis is usually good. However, cases with associated chromosomal,
prematurity and cardiac defects are at increased risk of death.
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer
These items normal warranty are two years, however the warranty doesn’t cover “wear and tear”. The manufacturer does have 100% quality control on these models.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
Related Products

$456.00
Was $507.00
3D Printed Carcinoma of Larynx with a 13 Month History of Dysphonia
Item # MP2052


$473.00
Was $526.00
3D Printed Intussusception of Small Bowel Due to Metastatic Tumour
Item # MP2077



























by — Item # MP2059
3D Printed Tracheoesophageal Fistula and Oesophagus Atresia
$281.00
$313.00
Add to Cart
Add to Quote





























