

Your shopping cart is empty.
3D Printed Renal Cell Carcinoma


 Handling Guidelines for 3D Printed Models
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer

















































6.0 lb





🎄 HOLIDAY SAVINGS - Ends Dec 31 🎄
Discount has been automatically applied for this item.
3D Printed Renal Cell Carcinoma
Item # MP2097
$711.00
$790.00
You save $79.00
Need an estimate?
Click Add To Quote

Features & Specifications
-
 by
by
A trusted GT partner -
 3D Printed Model
3D Printed Model
from a real specimen -
 Gov't pricing
Gov't pricing
Available upon request
 by
by 
Frequently Bought Together

3D Printed Renal Cell Carcinoma
Clinical History
A 64-year old male presents with a 5-month history of generalised malaise,
weight loss and dull right flank pain. On examination, there is a palpable right sided abdominal mass. He is noted
to be hypertensive. Urinalysis reveals microscopic haematuria. The patient underwent right nephrectomy.
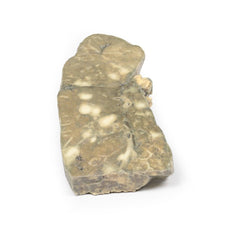
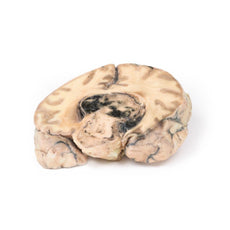
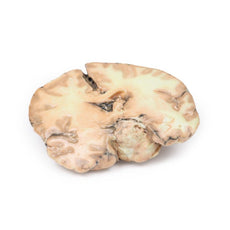
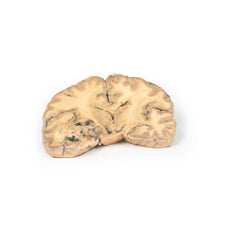
Pathology
The specimen is a kidney, which has been incompletely dissected in the coronal plane,
and mounted to display the cut surface. The lower pole of the kidney has been replaced by a rounded ill-defined
irregular mass 5cm in diameter, which has compressed and distorted the overlying renal parenchyma. The cut surface
of the tumour has a variegated appearance caused by areas of haemorrhage and necrosis. Several small pale-yellow
tumour nodules are present in the cortex and medulla above and separate from the lower pole tumour. These are
intrarenal metastases. The renal pelvis appears slightly dilated with some blunting of the renal papillae,
suggesting a degree of hydronephrosis. The capsular surface is finely nodular with a few coarse scars and contains
several small simple cysts (see rear of specimen). Histologically, the tumour was diagnosed as a renal cell
carcinoma.
Further Information
Renal cell carcinoma (RCC) comprise 85% of the primary renal malignancies.
They originate within the renal cortex. The risk of developing RCC is doubled in males. It most commonly occurs in
the 6th decade of life. Other risk factors for RCC include smoking, obesity, hypertension, unopposed estrogen
therapy, as well as exposure to asbestos, petroleum and heavy metals. Most RCC are sporadic but around 5% are due to
autosomal dominant familial cancers, such as Von Hippel Lindau syndrome, hereditary leiomyomatosis and
Birt-Hogg-Dubé syndrome.
There are several major primary renal tumour types according to genetic and histological tumour characteristics:
clear cell carcinoma (70-80%), papillary carcinoma (10-15%), chromophobe carcinoma (5-10%), oncytic carcinoma (3-7%)
and collecting (Bellini) Duct carcinoma (<1%).
Clear cell carcinoma typically have a deletion of chromosome 3p
and arise from the proximal tubule. They may be solid or less commonly cystic. They occur in association with Von
Hippel Lindau as well as sporadically. Papillary carcinomas arise from the proximal tubule. They are associated with
trisomies 7 and 17; loss of Y in male patients; and MET kinase domain mutations. They are frequently multifocal in
origin. Chromophobe carcinoma originate from intercalated cells of the collecting ducts. They are associated with
multiple chromosome losses and hypodiploidy. They have a low risk of disease progression.
Renal oncocytic
carcinomas are typically comprised of well-differentiated cells with prominently eosinophilic granular cytoplasm;
they are associated with a good prognosis. In contrast, collecting (Bellini) duct carcinoma of the kidney is a
highly aggressive tumour with an extremely poor prognosis as it does not respond well to chemotherapy drugs used for
renal cell carcinoma, and progresses and spreads more quickly. It is a variety of renal cell carcinoma (RCC) arising
from the distal segment of the collecting ducts of Bellini in the renal medulla.
The typical clinical features of RCC are costovertebral pain, palpable mass and haematuria. RCC is the great mimic in
medicine producing many manifestations including: polycythemia, hypercalcaemia, hypertension, pyrexia, Cushing‘s
syndrome, eosinophilia and amyloidosis. RCC tend to metastasize before producing may local symptoms. The most common
sites of distal spread are the lungs (50%) and bones (33%) followed by lymph nodes, adrenal glands and brain. RCC
has a tendency to invade
the renal vein and extend up it as a tumour thrombus, growing as a solid column
extending upto the inferior vena cava.
Ultrasound and CT are the most common investigations used to assess renal lesions and diagnose RCC. A tissue biopsy
may be required in some patients. An increasing number of patients are being diagnosed with RCC because of
incidental kidney lesions being detected on abdominal CT requested for other medical reasons.
The average 5-year
survival rate for RCC is 70%. Treatment depends on the stage of the tumour. Radical nephrectomy is the usual
surgical option. Medical treatment includes chemotherapeutic drugs as well as Vascular endothelial growth factor
(VEGF) inhibitors and tyrosine kinases inhibitors in patients with metastatic disease.
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer
These items normal warranty are two years, however the warranty doesn’t cover “wear and tear”. The manufacturer does have 100% quality control on these models.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
Related Products

$1,063.00
$1,182.00
Free shipping
3D Printed Shoulder with deep dissection of the left shoulder
Item # MP1525





























by — Item # MP2097
3D Printed Renal Cell Carcinoma
$711.00
$790.00
Add to Cart
Add to Quote
