

Your shopping cart is empty.
3D Printed Right Lung Military Tuberculosis


 Handling Guidelines for 3D Printed Models
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer

















































0.0 lb





🎄 HOLIDAY SAVINGS - Ends Dec 31 🎄
Discount has been automatically applied for this item.
3D Printed Right Lung Military Tuberculosis
Item # MP2060
$747.00
$830.00
You save $83.00
Need an estimate?
Click Add To Quote

Features & Specifications
-
 by
by
A trusted GT partner -
FREE Shipping
U.S. Contiguous States Only -
 3D Printed Model
3D Printed Model
from a real specimen -
 Gov't pricing
Gov't pricing
Available upon request
 by
by 
Frequently Bought Together

3D Printed Right Lung Military Tuberculosis
Clinical History
A 74-year old male presented with increasing shortness of breath and
haemoptysis. Further history reveals 20kg weight loss in 6 months, night sweats and a chronic cough. He has recently
moved from a country where TB is endemic. On examination, he has hypoxic and tachypnoea and has bilateral
crepitations throughout his lung fields and a dull left lung base on percussion. His quantiferon gold blood test is
positive. His chest x-ray showed bilateral small nodular deposits and a left basal pneumonia. He died from
respiratory failure soon after admission.
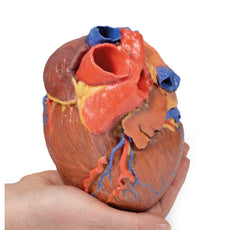
Pathology
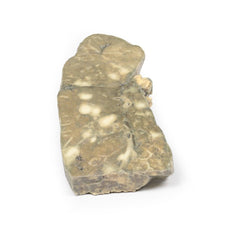
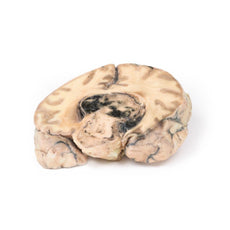
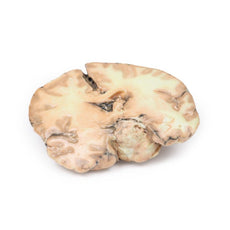
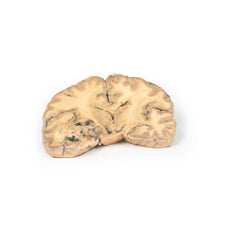
The right lung has been sliced longitudinally and mounted to display the cut surface.
The bronchi and bronchioles are mildly ectatic. Scattered throughout the entire lung parenchyma are large numbers of
small, pale yellows nodules less than 1 mm in diameter. Similar tiny subpleural nodules are seen on the surface of
the visceral pleura. The nodules are tubercles. This is miliary tuberculosis, so-called due to the resemblance of
the nodules to millet seeds.
Further Information
Tuberculosis (TB) is a chronic pulmonary and systemic infectious disease
caused by Mycobacterium tuberculosis. Transmission most commonly occurs via inhalation of aerosolized droplets of
this pathogenic bacteria, first described by Robert Koch (1882). Risk factors for contracting TB include being an
inhabitant of a developing country where the disease is endemic, immunosuppression (e.g. HIV, steroid use, anti-TNF
use and diabetes), chronic lung disease (e.g. silicosis), alcoholism and malnutrition.
After initial pulmonary
infection of M. tuberculosis clinical manifestation varies. In 90% of individuals with an intact immune system they
enter an asymptomatic latent infection phase. This latent TB may reactivate at any time in the patient‘s life. In
the other 10% of patients, especially in the immunocompromised, they develop primary disease which is immediate
active TB infection. Manifestations of primary TB include pulmonary infection symptoms (e.g. consolidation, effusion
and hilar adenopathy) and extra pulmonary symptoms including lymphadenopathy, meningitis and disseminated miliary
TB.
Secondary tuberculosis occurs when there is reactivation of previous latent TB infection. Around 10% of
latent TB will reactivate usually during periods of weakened host immunity. Typical symptoms of reactivation are
cough, haemoptysis, low grade fever, night sweats and weight loss.
Miliary TB occurs when the mycobacterium
erodes into a pulmonary vein and seeds elsewhere. The organism can circulate back to the lung and disseminate
thought the lung parenchyma as in this case. Systemic miliary tuberculosis can occur when the mycobacterium is
disseminated through the arterial system. The TB can then deposit in any organ but most commonly in the liver, bone
marrow, spleen and adrenal glands.
The immune response against TB is mediated via TH1 cells stimulate alveolar macrophages to attack the mycobacteria.
These macrophages surround the infection forming a granuloma surrounding a central area of ‘caseous’ (white
cheese-like) necrosis. Secondary pulmonary TB may heal with fibrosis or progress as in this case. Progressive
pulmonary TB sees erosion and expansion of the infectious lesion into adjacent lung parenchyma. This leads to
evacuation of the caseous centre leading to fibrous cavitation. Erosion of blood vessels can occur causing
haemoptysis. Post treatment of TB the tissue heals by fibrosis but does not recover the pulmonary
architecture.
TB diagnosis is usually made with a clinical history and chest x-ray and multiple sputum cultures.
Mantoux skin tuberculin test and serum interferon gamma release assay may also be used to help screen for infection.
Biopsies may be taken of suspected infection site for culture to assist diagnosis. Treatment involves prolonged
courses of multiple antibiotics, which depend on the antibiotic resistance of the infecting mycobacterium.
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer
These items normal warranty are two years, however the warranty doesn’t cover “wear and tear”. The manufacturer does have 100% quality control on these models.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
Related Products

$1,063.00
$1,182.00
Free shipping
3D Printed Shoulder with deep dissection of the left shoulder
Item # MP1525





























by — Item # MP2060
3D Printed Right Lung Military Tuberculosis
$747.00
$830.00
Add to Cart
Add to Quote
