

Your shopping cart is empty.
3D Printed Septic Renal Infarct


 Handling Guidelines for 3D Printed Models
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer

















































3.0 lb





🎄 HOLIDAY SAVINGS - Ends Dec 31 🎄
Discount has been automatically applied for this item.
3D Printed Septic Renal Infarct
Item # MP2098
$281.00
$313.00
You save $32.00
Need an estimate?
Click Add To Quote

Features & Specifications
-
 by
by
A trusted GT partner -
 3D Printed Model
3D Printed Model
from a real specimen -
 Gov't pricing
Gov't pricing
Available upon request
 by
by 
Frequently Bought Together

3D Printed Septic Renal Infarct
Clinical History
A 54 year old male patient presents with flank pain. He is an active
intravenous drug user. Further questioning reveals a history of intermittent haematuria, fevers, malaise and
vomiting. On examination he is hypertensive and pyrexic. Inspection of his limbs reveals Janeway lesions on his
extremities and track marks from recent IV drug use. A systolic murmur is found on auscultation of his chest. Blood
tests reveal elevated inflammatory markers, impaired renal function, elevated LDH and multiple bacteraemic blood
cultures. Echocardiogram shows a large mobile tricuspid vegetation. He was commenced on treatment for infective
endocarditis but later died from a sudden cardiac arrest.
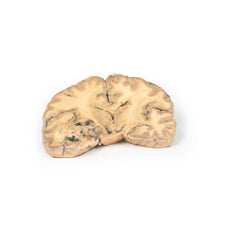
Pathology
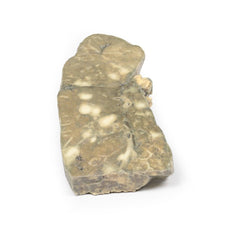
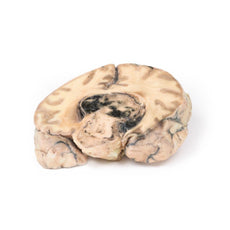
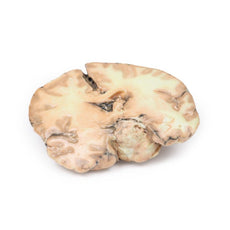
The specimen is the patient’s kidney from post mortem examination. The kidney has been
bisected with a cut half surface on display. There are multiple well demarcated wedge shaped pale yellow-white areas
evident within the cortex. The base of these pyramids lies against the cortical surface and extend along the renal
columns with the apex pointing toward the medulla. The largest is evident lateral upper pole of the kidney. Theses
pale areas are infarcted renal tissue. There are dark irregular shaped areas which represent areas of hemorrhage.
Further Information
Renal infarction results from an interruption in the blood flow to the
kidney. The kidneys receive almost a quarter of the cardiac output but have limited collateral circulation. The
cortex is the most susceptible area to infarction given blood supply is from proximal to distal. The main causes of
interruption of this circulation are cardioembolic disease, renal artery damage, hypercoagulable states or
idiopathic.
Cardioembolic causes are the most common. These include post-myocardial infarction mural thrombi, septic emboli from
infective endocarditis and emboli from mechanical valves. Idiopathic renal infarction is the second most common
cause. Damage to the renal artery is the third most frequent cause and includes renal artery dissection, acute
vasculitis of polyarteritis nodosa, trauma or post endovascular intervention. Hypercoagulable states are the rarest
cause of renal infarcts such as hereditary thrombophilia and antiphospholipid syndrome. Infarction is bilateral in
~15% of cases.
Presentation of renal infarction depends on the underlying etiology. It can be clinically silent.
Common manifestations include costovertebral angle pain, haematuria, hypertension due to increased renin release,
nausea, vomiting and sometimes fever.
Laboratory test used to aid diagnosis include urinalysis for hematuria and
serum creatinine levels which may be elevated, especially in bilateral disease. CT abdomen with contrast is the
first choice radiological investigation. A wedge-shaped perfusion defect is the classic finding. Treatment varies
depending on the cause of the infarction but generally involves supportive therapy and treatment of the underlying
pathology.
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer
These items normal warranty are two years, however the warranty doesn’t cover “wear and tear”. The manufacturer does have 100% quality control on these models.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
Related Products

$1,063.00
$1,182.00
Free shipping
3D Printed Shoulder with deep dissection of the left shoulder
Item # MP1525





























by — Item # MP2098
3D Printed Septic Renal Infarct
$281.00
$313.00
Add to Cart
Add to Quote
