

Your shopping cart is empty.
3D Printed Tuberculosis





 Handling Guidelines for 3D Printed Models
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer

















































3.0 lb





3D Printed Tuberculosis
Item # MP2111
$304.00
$338.00
You save $34.00
Need an estimate?
Click Add To Quote

Features & Specifications
-
 by
by
A trusted GT partner -
 3D Printed Model
3D Printed Model
from a real specimen -
 Gov't pricing
Gov't pricing
Available upon request
 by
by 
About This Item
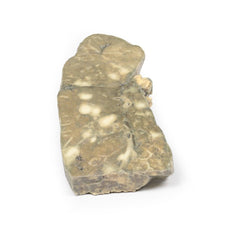
3D Printed Tuberculosis
Clinical History
A 37-year old female presents with increasing thoracic back pain. She has a
history of untreated human immunodeficiency virus (HIV) infection and pulmonary tuberculosis. History revealed
ongoing low-grade fevers, chills and weight loss. Examination revealed a cachexic patient with tender thoracic
vertebrae at multiple levels. Blood test showed an elevated serum calcium and erythrocyte sedimen
Frequently Bought Together
Total Price: $1,587.91 $1,529.91
- This item: 3D Printed Tuberculosis $338.00 $304.00
- Pediatric 4 Vessel Ultrasound Training Block $754.91
- Brayden CPR Training Manikin $495.00 $471.00
Total Price: $1,587.91 $1,529.91

3D Printed Tuberculosis
Clinical History
A 37-year old female presents with increasing thoracic back pain. She has a
history of untreated human immunodeficiency virus (HIV) infection and pulmonary tuberculosis. History revealed
ongoing low-grade fevers, chills and weight loss. Examination revealed a cachexic patient with tender thoracic
vertebrae at multiple levels. Blood test showed an elevated serum calcium and erythrocyte sedimentation rate. X-ray
of her spine showed lytic areas in the thoracic vertebrae. During her hospital admission, she developed urosepsis
and died.
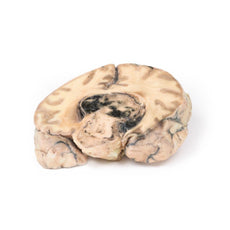
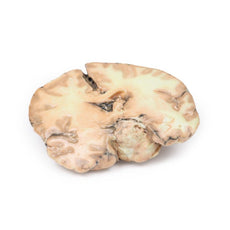
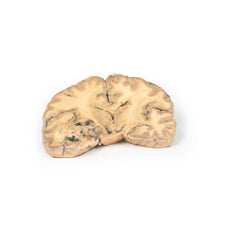
Pathology
The specimen is a portion of the patient’s thoracic vertebral column that has been
sawn longitudinally and mounted to display the cut surface of 7 thoracic vertebrae. In all vertebrae, there are
osteolytic areas, varying from 1 to 12 mm in diameter, which contain caseous degenerative material* (mostly now
lost) and are surrounded by a thin zone of dense bone. The tuberculous inflammatory process has extended into one of
the intervertebral discs, and has also spread outside the vertebral bodies to form collections of caseous material
beneath the anterior longitudinal ligament. This is an example of tuberculous mycobacterial osteomyelitis of the
vertebral column with paravertebral extension, also known as Pott’s Disease.
Further Information
Tuberculosis (TB) is a chronic pulmonary and systemic infectious disease
caused by Mycobacteria tuberculosis. Transmission most commonly occurs via inhalation of aerosolized droplets of M.
tuberculosis. Risk factors for contracting TB include being an inhabitant of a ‘developing’ country where the
disease may be endemic, immunosuppression (e.g. HIV, steroid use, anti-TNF use and diabetes), chronic lung disease
(e.g. silicosis), alcoholism, and generalized malnutrition.
After initial pulmonary infection of M. tuberculosis
clinical manifestation varies. In 90% of individuals with an intact immune system, they enter an asymptomatic latent
infection phase. This latent TB may reactivate at any time in the patient‘s life. In the other 10% of patients,
especially in the immunocompromised population, they develop primary disease, which is immediate active TB
infection. Manifestations of primary TB include pulmonary infection symptoms (e.g. consolidation, effusion and hilar
adenopathy) and extra pulmonary symptoms – lymphadenopathy, meningitis and disseminated miliary TB. Secondary
tuberculosis occurs when there is reactivation of a previous latent TB infection. Around 10% of latent TB will
reactivate usually during periods of weakened host immunity. Typical symptoms of reactivation are cough,
haemoptysis, low grade fever, night sweats and weight loss.
Osseous infection occurs 1-3% of patients with TB infection. There is a higher incidence of developing bone disease
in patients from developing countries and immunocompromised patients. The TB usually spreads haematogenously from
the site of active disease. Pott’s disease accounts for 40% of TB bone infections. The infection is destructive
eroding vertebral discs and vertebrae leading to compression fractures, which may cause symptoms of cord or nerve
root compression. Symptoms include pain at the site of disease, fevers, chills, weight loss, symptoms of compression
and spinal deformities, such as kyphosis and scoliosis.
TB diagnosis is usually made with a clinical history and
chest x-ray and multiple sputum cultures. Mantoux skin tuberculin test and serum interferon gamma release assay may
also be used to help screen for infection. Biopsies may be taken of suspected infection site for culture to assist
diagnosis.
Treatment involves prolonged courses of multiple antibiotics, which depend on the antibiotic
resistance of the infecting mycobacterium species.
* Caseous degeneration or necrosis is a unique form of cell
death in which the tissue maintains a cheese-like appearance.
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer
These items normal warranty are two years, however the warranty doesn’t cover “wear and tear”. The manufacturer does have 100% quality control on these models.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
Related Products



$1,880.00
Was $2,089.00
3D Printed Foot with deep structures of the distal leg and foot
Item # MP1930



$456.00
Was $507.00
3D Printed Carcinoma of Larynx with a 13 Month History of Dysphonia
Item # MP2052

$473.00
Was $526.00
3D Printed Intussusception of Small Bowel Due to Metastatic Tumour
Item # MP2077























by — Item # MP2111
3D Printed Tuberculosis
$304.00
$338.00
Add to Cart
Add to Quote
















