

Your shopping cart is empty.
3D Printed Pericardial Space


 Handling Guidelines for 3D Printed Models
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer

















































0.0 lb







🎄 HOLIDAY SAVINGS - Ends Dec 31 🎄
Discount has been automatically applied for this item.
3D Printed Pericardial Space
Item # MP1121
$3,011.00
$3,346.00
You save $335.00
Need an estimate?
Click Add To Quote

Features & Specifications
-
 by
by
A trusted GT partner -
FREE Shipping
U.S. Contiguous States Only -
 3D Printed Model
3D Printed Model
from a real specimen -
 Gov't pricing
Gov't pricing
Available upon request
 by
by 
Frequently Bought Together

3D Printed Pericardial Space
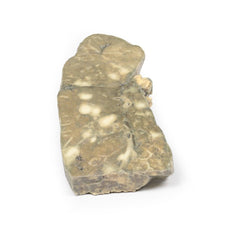
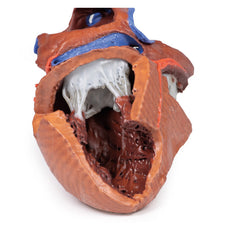
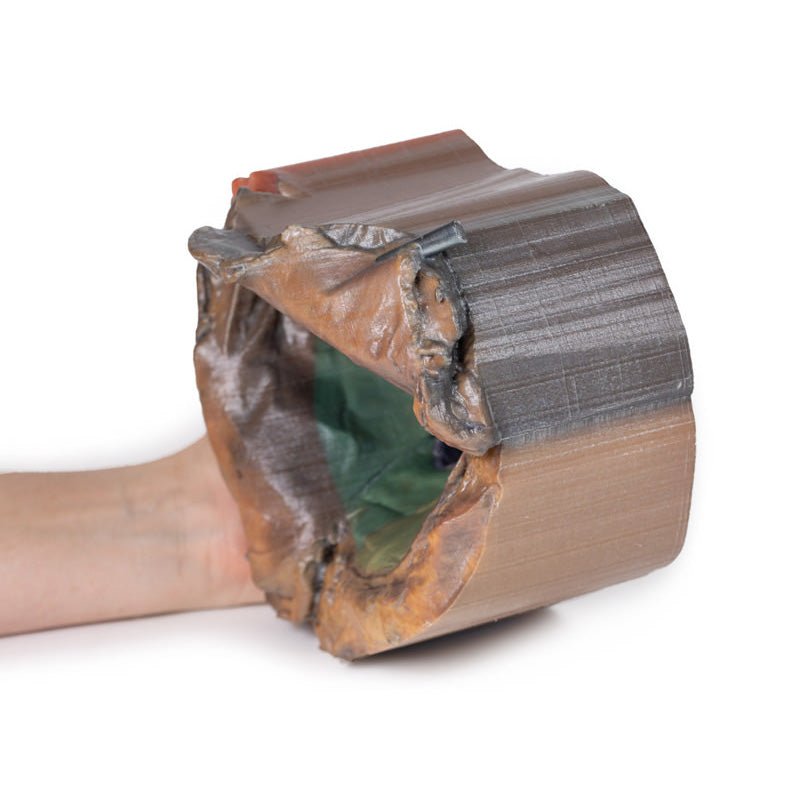
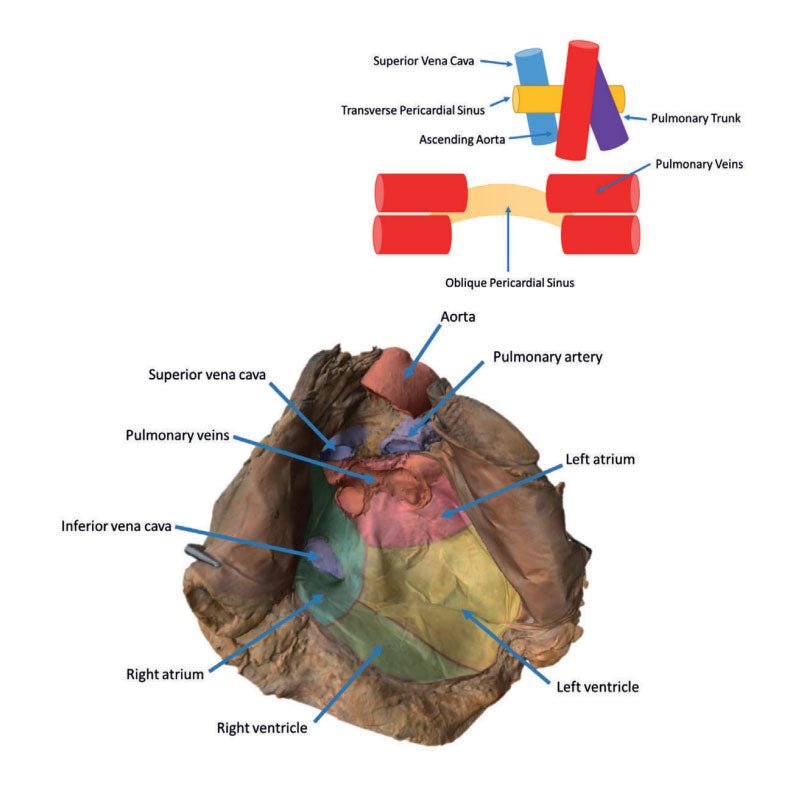
In this specimen the heart itself has been removed to demonstrate the reflections of parietal peritoneum and the orientation of the heart relative to other structures, including the diaphragm (diaphragmatic surface) and the lungs (left and right pulmonary surfaces). The pericardium is the multilayered fibroserous sac that encloses the heart and is continuous with the serous visceral pericardium (epicardium) of the heart itself. In normal anatomical position, the boundaries of the parietal pericardium are also the boundaries of the middle mediastinum (what we call coterminous). The internal surface of the parietal peritoneum has been false coloured to aid in identifying the regions of the heart that are normally positioned in these parts of the middle mediastinum.
The base of the heart is roughly rectangular and projects superiorly and posteriorly (anterior to the hilum of the lungs). It can be seen on the model as the most posterior surface left by the impression of the heart. It is formed by the left atrium (pink) (and to a lesser extent the right atrium [blue-green]) and the proximal parts of the great vessels (red and blue) as they enter and leave the heart. This is also the ‘fixed’ region of the heart, anchoring the heart through the origins of the great vessels where the visceral and parietal serous pericardium are reflected and continuous. The transverse pericardial sinus (clinically relevant for some cardiac surgical procedures) is visible between the pulmonary arteries (red) and the bases of the superior vena cava, pulmonary trunk, and ascending aorta. Inferior to the pulmonary veins, the depressed region formed by the left atrium and left ventricle is termed the oblique pericardial sinus.
From the base, the heart projects anteriorly, inferiorly and towards the left side of the thorax. The most inferior and lateral point is the apex. The apex is formed by the inferolateral part of the left ventricle (yellow) and is normally found in the left fifth intercostal space along the midclavicular line.
Within the mediastinum, the heart rests on the diaphragmatic surface, consisting mainly of left ventricle (and to
a lesser extent the right ventricle [light green]). This is the most inferior aspect of the heart and is
separated from the base (the posterior surface) by the coronary sinus. It extends from the base of the heart to
its apex. On the model it is the area that is just anterior and inferior to the ostium of the inferior vena
cava.
The pulmonary surfaces are the broad and convex right and left lateral sides of the heart. The left pulmonary
surface reflects onto the left lung and consists mainly of the left ventricle. The right pulmonary surface
reflects onto the right lung and consists of the right atrium.
The heart also has an anterior surface that consists mostly of the right ventricle with some right atrium on the
right and left ventricle on the left. In this model this surface cannot be appreciated as it has been dissected
deep to the anterior surface. The portion of the pericardium that can be seen being reflected to either side
would have covered, in part the anterior surface before they were reflected.
Great Vessels
The aorta carries oxygenated blood from the heart into the systemic circulation. It begins as the ascending
aorta and originates from the aortic orifice at the base of the left ventricle of the heart. The left and right
coronary arteries branch off immediately superior to the aortic orifice from the left and right aortic sinuses
respectively to supply the heart muscle itself. The vessel moves superiorly to the level of the second right
costal cartilage, the sternal angle, and is then referred to as the arch of the aorta. It becomes the descending
or thoracic aorta when the arch moves inferiorly to the vertebral level T4. It spans down to T12 level and
supplies much of the thorax.
The superior vena cava is a large vein is formed primarily by the union of the right and left brachiocephalic
veins. It drains directly into the right atrium at the SVC ostium, carrying a significant portion of
deoxygenated blood of the upper body.
The inferior vena cava is another large vein that drains much of the deoxygenated blood of the lower body, with
many tributaries contributing to it throughout the trunk. It drains directly into the right atrium at the IVC
ostium.
Pulmonary Vessels
The pulmonary trunk arises from the right ventricle of the heart. It bifurcates to give rise to the left and
right pulmonary arteries left of the midline just inferior to vertebral level T4/5 and the arch of the aorta.
These carry deoxygenated blood to the lungs, entering at the root of the lung in the hilum.
There are four pulmonary veins in total. A superior and inferior pulmonary vein for each side, left and right.
They carry oxygenated blood from the lung, beginning at the hilum and passing through the root of the lung, to
the left atrium of the heart.
Transverse and Oblique Pericardial Sinus
The transverse sinus can be described as the common point of parietal and visceral pericardium. This is located
beneath the aorta and pulmonary trunk and depicts a tunnel.
In contrast to the tunnel-like transverse sinus, the oblique pericardial sinus is more like an ocean bay. The
two types of pericardium here also meet, and it is located between the pulmonary veins.
Handling Guidelines for 3D Printed Models
GTSimulators by Global Technologies
Erler Zimmer Authorized Dealer
These items normal warranty are two years, however the warranty doesn’t cover “wear and tear”. The manufacturer does have 100% quality control on these models.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
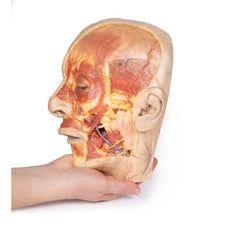
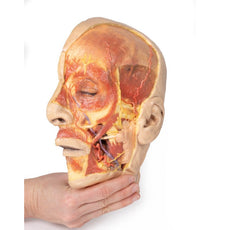
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
The models are very detailed and delicate. With normal production machines you cannot realize such details like shown in these models.
The printer used is a color-plastic printer. This is the most suitable printer for these models.
The plastic material is already the best and most suitable material for these prints. (The other option would be a kind of gypsum, but this is way more fragile. You even cannot get them out of the printer without breaking them).The huge advantage of the prints is that they are very realistic as the data is coming from real human specimen. Nothing is shaped or stylized.
The users have to handle these prints with utmost care. They are not made for touching or bending any thin nerves, arteries, vessels etc. The 3D printed models should sit on a table and just rotated at the table.
Related Products

$1,063.00
$1,182.00
Free shipping
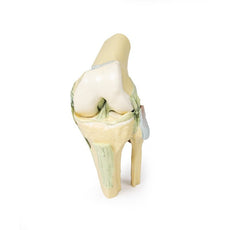
3D Printed Shoulder with deep dissection of the left shoulder
Item # MP1525





























by — Item # MP1121
3D Printed Pericardial Space
$3,011.00
$3,346.00
Add to Cart
Add to Quote
